
Lumbar TLIF – OPEN/MIS
A transforaminal lumbar interbody fusion (TLIF) is performed to remove a portion of a disc that is the source of back or leg pain. Like the PLIF (posterior lumbar interbody fusion) procedure, bone graft is used to fuse the spinal vertebrae after the disc is removed. However, the TLIF procedure places a single bone graft between the vertebrae from the side, rather than two bone grafts from the rear as in the PLIF procedure. Inserting the graft from the side where the facet joint has been removed is an effort to avoid moving or damaging nerve roots during the procedure.
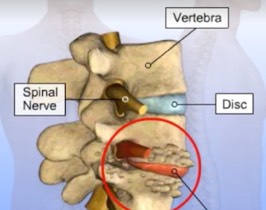
An incision is made in the middle of the low back. Surgical instruments are used to remove the entire facet joint on one side in order to allow access to the degenerated disc. A grasping instrument is used to remove most of the intervertebral disc. Removing the facet joint and disc relieves pressure on the compressed spinal nerve, allowing it to return to the proper position.
A single bone graft is placed in the disc space from the lateral (side) aspect through the area exposed when the facet joint was removed. The bone graft will provide stability to the spine when it fuses with the vertebrae above and below it. In variations of this procedure, spacers, cages packed with graft material, or ground bone graft material may also be packed into the disc space to aid with the fusion.
To prepare for additional fusion along the transverse processes, which will further stabilize the vertebrae, a motorized instrument is used to remove the top (cortical) layer of the transverse processes. This is the site where the bone grafts for the new fusion will be added.
Before bone grafts are added, instrumentation is introduced to stabilize the spine. A drill is used to make holes in the pedicle area of the vertebrae, and screws are placed in the drilled holes. Next, rods are positioned between the screws and fastened in place. The rod and screw instrumentation provides stability to the spine and prevents the vertebrae from moving while the bone graft fusion takes place.
Bone grafting can be done with pieces of a patient’s own bone (autograft), processed bone from a bone bank (allograft), or a bone graft substitute (demineralized bone, ceramic extender, or bone morphogenetic protein). To harvest a patient’s own bone for grafting, a second incision is made over the back of the pelvis. Bone is removed from the iliac crest and placed along the prepared site where the top layer of bone was removed. This bone eventually grows in place, fusing the spine and providing additional stability.
The incisions are closed and dressed to complete the procedure. Adding the instrumentation with bone graft fusion increases the strength of the spine directly after surgery, and may decrease the need for a post-operative brace. Patients often remain in the hospital for two to four days following the procedure and should avoid heavy lifting, bending, twisting, and turning for six to twelve weeks.